Reacted Magnesium provides three unique forms of highly-absorbed magnesium to ensure maximum absorption of this important macromineral. Most magnesium supplements use only a single-source of magnesium, which can easily overwhelm a single pathway of absorption, and limit uptake of high-dose magnesium regimens. Reacted Magnesium takes advantage of three unique pathways of absorption by providing magnesium as di-magnesium malate, magnesium citrate and magnesium glycinate for enhanced absorption, improved utilization and gastrointestinal (GI) comfort. Some individuals, who take other forms of magnesium supplements, often experience GI side effects, including gas, bloating, diarrhea, constipation or a combination of these symptoms. The forms of magnesium used in Reacted Magnesium preserve GI comfort while maximizing absorption and restoring magnesium levels in the body.
Overview
Magnesium is an abundant mineral in the body and is found naturally in many foods, like green leafy vegetables. It is also found in over-the-counter medications, such as laxatives. The average American intake of magnesium, according to the National Health and Nutrition Examination Survey (NHANES Study) is critically low: Many Americans fail to consume the estimated average requirement (EAR) established by the Institute of Medicine.[1] In addition, more than 57 % of the population does not meet the United States Department of Agriculture requirements for magnesium in the diet. Intracellular magnesium levels are decreased by excessive intake of alcohol, salt, coffee, phosphoric acid found in sodas, diets high in calcium and high stress levels. [2] Because of widespread nature of magnesium deficiencies, adequate daily intake of magnesium is critical for proper hydration, stress response, muscle relaxation, promoting healthy blood pressure levels, optimal bone mineral density, and blood sugar regulation. [3,4]
Bioavailability – The Mineral Chelate Difference
The importance of bioavailability is obvious. If consuming a magnesium supplement has little effect on improving the body’s magnesium balance, there is no reason to ingest it. Signs of inferior mineral supplements include the use of cheap, poorly absorbed, rock-salt minerals like calcium carbonate and magnesium oxide (See Figure 1). These mineral forms slow and limit absorption, relying on adequate stomach acid to release magnesium ions which then enter the body via passive diffusion. And, because they tend to remain in the intestines longer, these forms of mineral supplements can cause intestinal distress such as constipation (calcium carbonate) or diarrhea (magnesium oxide).
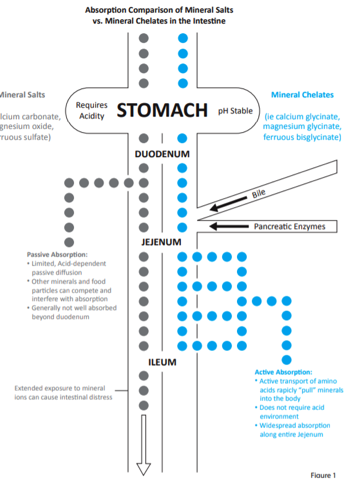
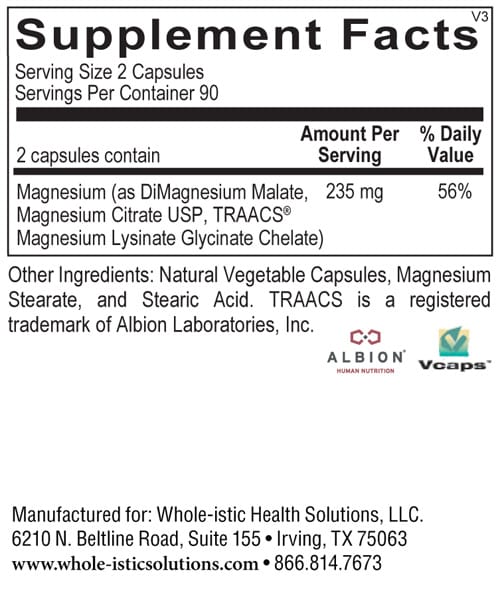
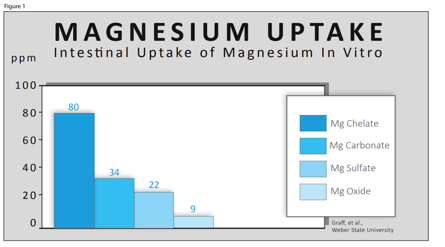
Reacted Magnesium provides the additional benefit of highlyabsorbed, Albion® mineral chelates. Albion® is the world leader in manufacturing highly bioavailable mineral chelates, a specialized form of minerals bound to amino acids. This patented process creates organic mineral compounds which use active absorption mechanisms in the gastrointestinal tract to greatly enhance mineral absorption. In a magnesium comparison study reported by Graff et al. at Weber State University, Albion®’s magnesium amino acid chelate had (See Figure 1)[5]:
- 8.8 times greater absorption than magnesium oxide
- 5.6 times greater absorption than magnesium sulfate
- 2.3 times greater absorption than magnesium carbonate
In addition, other comparison studies have shown significantly superior absorption of magnesium chelates compared to other mineral forms:
- At a dose of 400 mg, magnesium chelate significantly reduced or eliminated menstrual abdominal discomfort [6]
- Multiple double blind studies found urinary excretion of magnesium chloride higher than magnesium glycinate, proving superior absorption[7-9]
- Magnesium glycinate is shown to have a reduced laxative effect when compared to other forms of magnesium [10]
Mineral chelates are gentle, gut “friendly” minerals that do not cause diarrhea that often accompanies magnesium oxide and other rock-salt forms. Albion®’s mineral chelates have extensive clinical research proving their superior bioavailability, biologic activity, stability, and improved tolerance.
Heart Health
Studies to date have found that magnesium supplementation maintains healthy blood pressure levels.[11] Calcium is essential to the contraction of muscles, while magnesium aids muscle relaxation. Insufficient magnesium levels can contribute to constriction of the muscles in blood vessels and trigger changes in blood pressure levels. Several prospective studies have examined associations between magnesium intake and heart health. A systematic review and meta-analysis of prospective studies found that higher serum levels of magnesium were significantly associated with enhanced heart health and optimized blood flow to the heart. [12]
Insulin Balance
Magnesium is integral for the transport of insulin from the bloodstream to cells. Increasing magnesium levels has been shown to maintain normal blood sugar levels. Diets with higher amounts of magnesium are associated with blood sugar balance, due to the role of magnesium in glucose metabolism. [13-15] Most investigations of magnesium intake and insulin balance have been prospective cohort studies. A meta-analysis of seven of these studies, which included 286,668 patients, found that a 100 mg/day increase in total magnesium intake promoted insulin balance by a statistically significant 15%. [10] Another meta-analysis of eight prospective cohort studies that followed 271,869 men and women for an extended period of time found a significant association between magnesium intake from food and insulin balance.[16]
Bone Health
Magnesium is involved in bone formation and influences the activity of osteoblasts and osteoclasts, cells responsible for the breakdown and formation of bone. [17] Magnesium also impacts concentrations of parathyroid hormone and the active form of vitamin D, which are major regulators of bone homeostasis. Several population-based studies have found positive associations between magnesium intake and the state of bone strength and mineralization in men and women.[18-19]
Directions
2 or more capsules per day or as recommended by your health care professional.
Does Not Contain
Gluten, corn, yeast, artificial colors and flavors.
Cautions
If you are pregnant or nursing, consult your physician before taking this product.
References
1. Moshfegh A, Goldman J, Ahuja J, Rhodes D, LaComb R. 2009. What We Eat in America, NHANES 2005-2006: Usual Nutrient Intakes from Food and Water Compared to 1997 Dietary Reference Intakes for Vitamin D, Calcium, Phosphorus, and Magnesium. U.S. Department of Agriculture, Agricultural Research Service.
2. Johnson S. The multifaceted and widespread pathology of magnesium deficiency. Med Hypotheses 2001; 56(2): 163-70.
3. Ryder KM, Shorr RI, Bush AJ, Kritchevsky SB, Harris T, Stone K, Cauley J, Tylavsky FA. Magnesium intake from food and supplements is associated with bone mineral density in healthy older white subjects. J AM Geriatr Soc 2005; 53(11):1875-80.
4. Gobbo LCD, Imamura F, Wu JH, Otto MCO, Chiuve SE, Mozaffarian D. Circulating and dietary magnesium and risk of cardiovascular disease: a systematic review and meta-analysis of prospective studies. Am J Clin Nutr 2013; published online May 29, 2013.
5. Graff et al. Magnesium: wide spread benefits. Albion Research Notes 1992; 1(2):1.
6. Abraham GE, Primary dysmenorrhea, Clin Ob Gyn, 21:139-145, 1978.
7. Abrams SA, et al., Advances in Magnesium Research Nutrition and Health, Op Cit, 109-114, 2001.
8. Schuette SA, Lashner BA, Janghorbani IY. Bioavailability of Magnesium diglycinate vs. magnesium oxide in patients with ileal resection. J Parent Ent Nutr, 18:430-435, 1994.
9. Roussouw J, Brummelen R. The bioavailability of four magnesium preparations. Publication pending.
10. Institute of Medicine (IOM). Food and Nutrition Board. Dietary Reference Intakes: Calcium, Phosphorus, Magnesium, Vitamin D and Fluoride. Washington, DC: National Academy Press, 1997.
11. Rude RK. Magnesium. In: Coates PM, Betz JM, Blackman MR, Cragg GM, Levine M, Moss J, White JD, eds. Encyclopedia of Dietary Supplements. 2nd ed. New York, NY: Informa Healthcare; 2010:527-37.
12. Rude RK. Magnesium. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease. 11th ed. Baltimore, Mass: Lippincott Williams & Wilkins; 2012:159-75.
13. Dickinson HO, Nicolson D, Campbell F, Cook JV, Beyer FR, Ford GA, Mason J. Magnesium supplementation for the management of primary hypertension in adults. Cochrane Database of Systematic Reviews 2006: CD004640.
14. Del Gobbo LC, Imamura F, Wu JHY, Otto MCdO, Chiuve SE, Mozaffarian D. Circulating and dietary magnesium and risk of cardiovascular disease: a systematic review and meta-analysis of prospective studies. Am J Clin Nutr 2013;98:160-73.
15. Larsson SC, Wolk A. Magnesium intake and risk of type 2 diabetes: a meta-analysis. J Intern Med 2007;262:208-14.
16. Rodriguez-Moran M, Simental Mendia LE, Zambrano Galvan G, Guerrero-Romero F. The role of magnesium in type 2 diabetes: a brief based-clinical review. Magnes Res 2011;24:156-62.
17. Schulze MB, Schulz M, Heidemann C, Schienkiewitz A, Hoffmann K, Boeing H. Fiber and magnesium intake and incidence of type 2 diabetes: a prospective study and meta-analysis. Arch Intern Med 2007;167:956–65.
18. Rude RK, Singer FR, Gruber HE. Skeletal and hormonal effects of magnesium deficiency. J Am Coll Nutr 2009;28:131–41.
19. Tucker KL. Osteoporosis prevention and nutrition. Curr Osteoporos Rep 2009;7:111-7.